The most effective source of carbon-free energy available on a large scale is nuclear and this would be accepted but for the general view that it is particularly dangerous. The scientific evidence does not support this long-held apprehension. Why has this contradiction persisted for so long and why is nuclear power apparently so expensive? The evidence makes plain the need for a root-and-branch cultural change in attitudes to nuclear technology.
1. Science and sociology
Science, like mathematics, should be objective and its truth should not involve social and political views. This goal is widely agreed and often achieved, but not always. Where social influences distort scientific truth, they also discourage the transparent examination of evidence from which correction should follow. A misunderstanding may then persist for a long time, as has happened to perceptions of nuclear energy.
Nuclear weapons create blast and fire, but as data from Hiroshima and Nagasaki now confirm radiation was not the significant cause of death that most people suppose. Nevertheless the politics of the Cold War and the nuclear arms race gave the words nuclear and radiation a fearsome meaning in the public mind, and thence for many scientists and politicians too. Such fear prevents understanding, and democracy fails when the electorate does not understand the issues. This makes it important to explain in accessible terms what the underlying biological and physical science has to say about nuclear safety.
Although I have worked with radiation and taught nuclear and medical physics courses at Oxford [AL2006], I have never had any link with the nuclear industry. This has given me the opportunity to study and express the issues with an independent voice and publish two books [AL2009, AL2015].
As I will explain, if nuclear power and its safety were understood in the same way as other risks, there would be no reason for it to be expensive. This is important because nuclear power can make a unique contribution as the basic source of energy and a main driver of a viable economic future without any impact on the environment. The science is not technically difficult but engaging with long held contrary opinion is harder. That is the problem that I will now address.
Firstly I discuss two alarms that are ringing: these indicate that our beliefs and the reasoning often given in support of them are mistaken. Secondly I explain some physical and biological aspects of what happens when radiation is absorbed by material, in particular living tissue. Next I summarise briefly the evidence for the effects of radiation, in particular on humans. Many people do not agree with my conclusions and I discuss briefly why this is so. The next question is how large can a radiation dose be and yet be quite harmless. Given the answer to this scientific question courts of law and regulations should rule any lesser exposure to be safe. That these doses are much higher than those allowed by current regulations leads to important conclusions.
2. An alarm call, the reaction to the Fukushima accident
The scale of the nuclear accident that followed the earthquake and tsunami in Japan on 11 March 2011. was evident in a couple of weeks [AL2011]. In September and October 2011 I visited the area, spoke with doctors, community leaders and school teachers to hear at first hand how residents and the authorities had responded to the nuclear accident.
Three separate things happened there in March 2011: the first was natural, the second was avoidable and the third unnecessary.
Firstly there was an exceptional earthquake and tsunami – a natural disaster with massive physical destruction that caused 18,800 deaths. However all Japanese people learn at school what they should do in the event of an earthquake. Remarkably thanks to this instruction, 96% of the 500,000 people in the region inundated by the tsunami escaped in the 30 mins between the earthquake and the arrival of the tsunami. Also as planned, all the nuclear power stations in Japan shut down immediately the earthquake struck.
Secondly three nuclear reactors at the Fukushima Daiichi plant were destroyed with fuel meltdown and a release of radioactivity. This happened because the emergency generators were sited low down on the sea side of the plant and were inundated by the tsunami: that was the avoidable mistake that caused the accident, but there were no casualties from the released radioactivity and none is expected in future. This should have been seen as no more than a local accident, not a disaster.
Thirdly there was local and worldwide panic caused by an excessive fear of radiation. There had been no programme of public education to prepare for a nuclear accident and the authorities were equally unprepared – such accidents were supposed not to happen. In the event, a hastily organised evacuation guided by excessively cautious safety standards itself caused 1600 extra deaths, food was condemned as contaminated, power stations were turned off on public safety concerns and replacement fossil fuel was imported. There was severe economic damage, reduced trust in society and in the ability of science to provide for people.
The radiation disaster itself that everyone expected never occurred but the wave of panic spread around the world on the back of ignorance and lost confidence. If the public had received a similar level of instruction and understanding about radiation that the people in Japan had about earthquakes and tsunamis, there would have been no consequences of global significance at all.
But other communication failures have added needlessly to the problem of confidence in science.
3. Another alarm, the credibility of published research
In a number of biomedical sciences published results are reported to be no longer widely believed. Naturally this threatens an implosion of confidence and trust, firstly within the science concerned and then more widely in society. These reports come from the editors of prestigious journals and are supported by a careful examination of a particular published result central to radiation biology.
Dr. Richard Horton, editor in chief of The Lancet, wrote [HO2016]
Much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with…an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness… In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world…Journal editors deserve their fair share of criticism too.… And individual scientists, including their most senior leaders, do little to alter a research culture that occasionally veers close to misconduct.
And Dr. Marcia Angell wrote [AN2009]
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.
These authoritative revelations are alarming and affect the credibility of many published reports of the health effects of ionising radiation. This is not true of all disciplines and great efforts are made in some “big” sciences to avoid such pitfalls, as discussed by Weidberg [WE2015].
Before looking at an example here is a draft list of checks that might reasonably be applied in any scientific field:
the statistical significance of a result should be several standard deviations (sd)1 – for example five, as for the recent discovery of gravitational waves and the Higgs Boson;
a result should be interpretable in terms of simple mechanisms;
a result should be compatible with other similar but larger experiments, if any.
An important result might reasonably fail one of these checks; any failing two of them should be seen as questionable; any failng all three would not be credible and therefore not publishable. Results that simply challenge orthodox science with ideas that have popular appeal should be held back until confirmed, otherwise science is brought into disrepute and everyone in society suffers through a loss of trust.
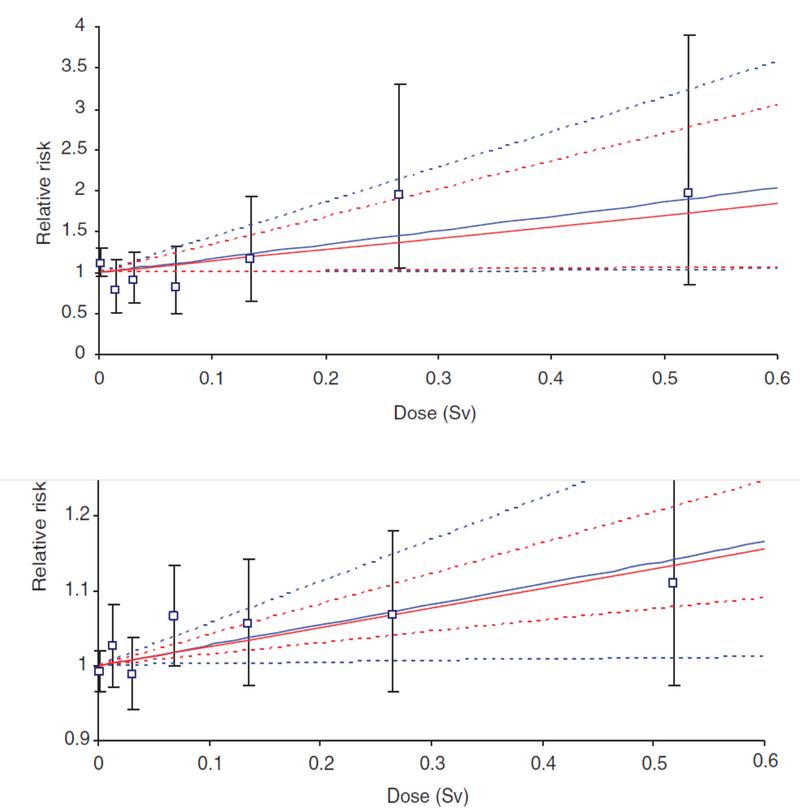
A simple but important example2 is taken from a paper by Muirhead et al [MU2009]. The plots in Figure 1 show cancer mortality of radiation workers against whole-of-life dose relative to those at zero dose. Do the data show that there is any significant dependence on this dose? The authors claim that the risk rises in a straight line from 1.0. The error flags show the 90% confidence limits given by the authors. So we might expect that 1 in 10 data points to lie out of line – that is what 90% confidence means. In fact on the leukaemia plot one of the seven data points nearly misses the horizontal line, Relative Risk = 1.0. That tells us that, if it is true that there is no dependence, then data such as these are quite likely - and this is the correct form of the statistical question: Is there significant evidence of a dependence? The lower plot shows the evidence for solid cancers and the story is similar there. In fact for both plots the claim made by Muirhead et al that there is a linear dependence fails all three of the general criteria suggested earlier:
the variations are consistent with random, as just discussed, so showing no evidence;
published data for those who live in geographical regions with high natural annual radiation dose rates show no dependence of cancer on dose rate, even where experienced over a life time;
there is no established mechanism on the basis of current radiobiology that would suggest a harmful effect of any such small chronic dose.
The unexamined influences on their data of smoking and the so-called Healthy Worker Effect reduce the credibility of their conclusion even further.
These data have reappeared recently as the dominant component of two meta analyses, one by Leuraud et al on leukaemia [LE2015] and the other by Richardson et al on solid cancers [RI2015]. These authors make the same claim for a dependence as Muirhead et al, although the same objections can be made. These published results have been independently and unfavourably reviewed by Sacks et al [SA2016] among others.
Perhaps we should not be surprised at the human tendency to see a result where none can be firmly established. Evolution favoured those who could spot danger lurking in the grass – and a few false alarms carried no penalty when survival was at stake in our early development. In science such enthusiastic hypothesising still plays a vital role behind the scenes but it has to be tempered by sceptical checking. Properly circumspect analyses put much effort into the simulation of experimental results by Monte Carlo and other means to verify that real uncertainties match the quoted confidence levels. But of similar importance is the need to understand how any conclusion matches – or does not – with existing knowledge, in this case of radiation absorption by living tissue.
4. The absorption of ionising radiation
The physics and chemistry of what occurs in the immediate aftermath of radiation absorption in matter have been carefully studied for over a century and are well understood. For a start, you might reasonably expect the material to get hot, as determined by the heating rate given by the number of watts of radiation power absorbed in each kg of material. Indeed the safety of ultrasound and MRI clinical scans is set in this way by comparison with the normal metabolic rate, a few watts per kg – this is the rate that the cooling mechanisms of living tissue are designed to disperse with relative ease. How many watts per kg are delivered by a typical ionising radiation exposure? By definition 1 gray of absorbed ionising radiation is 1 joule per kg. Therefore 1 watt per kg is 1 gray per sec, or 1000 mGy per sec. That would be a huge radiation dose rate although its heating is modest. A dose rate of 3 mGy per day, that is 1000 mGy per year, is only 32×10-9 watts per kg. It is no wonder that ionising radiation gives no sensation – its heating effect is far too weak.
That suggests that a radiation dose rate of a few mGy per second might be quite harmless which is quite untrue. What have we misunderstood? This problem was solved by Einstein in 1905 in his account of the Photoelectric Effect.3 He used the understanding of the new Quantum Theory (that Planck had introduced only a few years earlier) to explain that when ionising radiation is absorbed it does not happen uniformly but as a series of local flashes or pin pricks, often termed collisions to accentuate their individual nature. Each pin prick delivers enough energy to ionise an atom or break a molecule – on a scale4 of about 3 eV (or 5×10-19 joules). So in a CT scan the absorption of 10mGy involves about 2×1016 such energy pricks per kg. But in a kg there are about 5×1025 atoms. That means the proportion of atoms affected is only about 1 in 2500 million. So the picture is one in which a tiny proportion of atoms is severely disrupted – but the others not at all.
Current safety recommendations based on the Linear No-Threshold (LNT) theory assume living tissue suffers the same immediate radiation cell damage as if it were dead – and that is reasonable. But then in the name of precaution it dismisses the effectiveness of subsequent biological action [IC2007]. It considers that any initial damage, whenever and wherever it arises, is equally likely to cause a malignant DNA error that leads to subsequent cancer. If true, resulting disease would be in proportion to the absorbed radiation energy. This is the LNT picture, suggesting that all ionising radiation is harmful and that any dose of radiation should be kept as low as reasonably achievable (ALARA) in the name of caution.
What the LNT model ignores is that biology is about the behaviour of live tissue. The small number of important hit atoms form part of delicate responsive molecules and when the cry ouch! goes up there is a response within the cell and via chemical messaging from other cells too.
How the size of a radiation dose determines the subsequent disease rate is an example of a stress-failure relationship, also named a cause-and-effect or dose-response curve. In fundamental physical science the relation between cause and effect is often extremely simple, and linearity is a natural consequence [AL2009]. However, for other systems where design or evolution has played an essential role, a linear relation between cause and effect is exceptional – in particular wherever the response is designed for stability or has evolved not to fail.
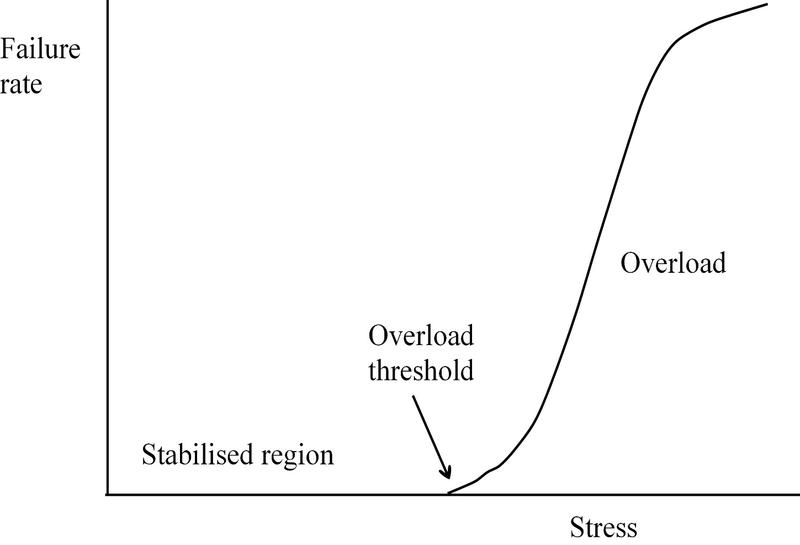
Figure 2 shows the type of curve that describes the failure rate of a stabilised system: for small stresses the failure rate is very small if not zero, because the stabilisation works. But it takes resources and time to react, so that a large sudden stress can cause overload such that failure becomes increasingly likely above a threshold. Such a curve for a resource-limited self protected system applies in situations as diverse as the handling of website traffic, business management, military strategy, chemical buffer solutions and electronic stabilisation.
It has been the business of biology for three billion years to evolve ways to stabilise life against failure as far as resources permit. If evolution had not found ways to protect life against ionising radiation, we would not be here, especially since radiation levels were somewhat higher on Earth at times in the past5. The protection required is against broken molecules which not only constitute damage themselves but may also go on to break further molecules. This process is called oxidation and the broken molecules reactive oxidant species (ROS). In fact it was important to evolve a similar strategy to protect life against the ROS leaked from mitochondria. These can also break molecules such as DNA.
To survive the effects of oxidation biology depends on its resilient design, its response to an immediate attack and its ability to adapt and modify that response in the light of experience:
-
an optimised design of life made up of many individuals, each replaced over many decades, and with each individual made up of many small cells, each replaced in a few weeks;
-
an effective response to an oxidative attack based on: 1) antioxidants to quench ROS; 2) enzymes to repair DNA; 3) arranged cell death (apoptosis); 4) suspension of the cell cycle to avoid copying DNA errors; 5) an immune system to police later rogue activity among cells;
-
an ability to adapt by providing sufficient enzymes and antioxidants using past stress levels.
Much is now known of these mechanisms and more is discovered every year. Resources are limited and it takes time to regroup and recovery from an attack. If too many cells die and are not replaced, organs fail and death by Acute Radiation Syndrome (ARS) follows. Alternatively if the imnune system fails a rogue DNA error may result in a tumour. Anyway the stabilisation depends on the radiation dose rate, rather than any value for accumulated dose in mGy. The importance of the dose rate is underlined by the effectiveness of protracted radiotherapy treatment (fractionation), as discussed later.
But the simple description given above is deceptive. The effect of adaptation is to increase the range of effective protection, meaning that the curve shown in Figure 2 changes. This happens when we take exercise and get fit and our tolerance to muscular stress is increased: this is not an analogy, but a real example of the way that cellular biology adapts to oxidative attack in the light of experience. As the failure threshold is increased the curve shifts to the right. Furthermore the added resources generally protect against other diseases too (each stress having its own curve). As is well known keeping fit provides extra protection against diseases such as cancer. This is a story about clever biology, and it is a mistake to try to reduce it to the simpleton mathematics of curves. Evidence that moderate X-ray exposures improve protection against subsequent larger doses was published as early as 1915 and 1920 – in that case the evidence was for mice but these defences are deep in our genetic make up and apply to most forms of life [MU1915, MU1920].
However, since the 1950s the international orthodoxy on the biological effects of radiation has been built on LNT. In that case the curve of Figure 2 is supposed to be by a straight line through zero, not plotted against dose rate but against total dose accumulated over a life time. That was tested in Figure 1 and failed. Clearly more evidence is needed to confirm the influence of active biology.
5. Further evidence
Although these basic features of cell biology and its defences against ionising radiation and other stresses go back billions of years and apply for most life forms, we are interested in data on human life in particular. Here we look at exposures of large numbers of people and high doses, namely in clinical medicine, the accident at Goiania (1987), the accident at Chernobyl (1986) and the record of the survivors of the bombs dropped on Hiroshima and Nagasaki (1945). Fuller details are given elsewhere [AL2009, AL2015]. Wider reading should include the recent accessible article by Henriksen and the Oslo Group [HE2016]. This discusses lung cancer and the chronic radiation dose rate to the lungs from natural radon gas.
The radiation used in medical clinics is the same in principle as that in accidents and nature. The steady natural background of radiation gives a dose rate between 2 and 100 mGy per year, depending mainly on altitude, geomagnetic latitude and the radioactivity of the local rocks. An acute dose of 10 mGy or less given in a diagnostic scan causes no demonstrable harm and is very small compared to the life-saving dose received by a patient on a course of radiotherapy. In that case the tumour cells receive 30 or more daily doses of 2000 mGy to kill them, while nearby healthy tissue gets 30 daily doses of about 1000 mGy and survives. This survivable dose, 30,000 mGy in a month, is about 10 times a dose that is usually fatal if delivered all in one day. This survival is due to the repair of DNA and other mechanisms discussed earlier. Successful cancer treatment is a compromise between too much radiation with the chance of triggering new disease and too little with the chance that the original tumour cells survive. Oncologists have a century of practical clinical experience of getting this balance right and the general public have taken part in this work, willingly and usually beneficially. There is no reason for suspicion – this information is not the product of some guinea-pig programme by the military, as some nuclear sceptics might suppose.
But a high dose of ionising radiation within a short time can be fatal. Four cases of early death from ARS were recorded at Goiania from whole-body acute doses between 4000 to 7000 mGy, and 28 deaths from such doses occurred at Chernobyl. At Fukushima there was no case of ARS, but there was widespread popular concern about internally absorbed radioactivity, in particular the volatile fission products, iodine-131 and caesium-137. The latter has a 30-year half-life and so persists in the environment although it is excreted from the body with a biological half-life of about 100 days. When the Fukushima accident occurred the effect of caesium-137 was known from what happened at Goiania [IA1988, IA1998]. The authorities at Fukushima, or at least the IAEA, should have told the public not to worry, but they did not. It takes years for bureaucracies to dare to respond, it seems, even with obvious answers to the most pressing questions based on data they already have.
At Goiania, Brazil, a caesium-137 therapy source of 50.9 tera-becquerels in an abandoned radiotherapy clinic was taken home by a scrap merchant and split open. He and his wife admired the pretty blue glow that the radiation created in the surrounding air. Their children played with it in the kitchen and got it onto their skin and into their food. Fascinated, they invited their neighbours in to see what they had found – then sold it to another family. After two weeks people started to get ill and then finally it was realised what had happened. Altogether 249 people had been significantly contaminated, more than 50 of them internally. Within a few weeks four had died of ARS and later 28 had surgical operations for burns. Having been scanned for internal caesium-137 and labelled irradiated many survivors suffered from depression, some becoming alcoholic – as happened again at Fukushima. But the internal contamination dose was quite different there: the least contaminated person who died at Goiania had 10,000 times the activity of the most contaminated person measured at Fukushima (out of 32,811 members of the public and 1,491 children). The important statistic is the number of internally contaminated members of the public at Goiania who died from radiation-induced cancer in the 25 years after the accident. The answer is zero [VA2013]. The number of survivors is small but this result would not be expected if internal irradiation by caesium-137 left any significant legacy of risk of cancer. This is the type of robust result we need – the number of radiation casualties at Fukushima is another.
What about those who survived Chernobyl? There were more of them, but is there any evidence that they incurred a continuing legacy of cancer after their exposure in 1986? The 237 fire fighters who were early on the scene received large doses from the exposed reactor core. As noted earlier 28 of these died from ARS in a few weeks. But what happened to the rest in later years? Inevitably some died anyway. Up to 2004 there were 19 deaths, but it has not been possible to show that these were associated with radiation [WH2006]. In fact there has been no confirmed evidence for additional cancer in 25 years, except 15 deaths from child thyroid cancer. However the dominant health effects have been mental and social. The human population was removed from their homes at short notice following the accident. Not knowing what was happening to them they suffered severely by being uprooted and cursed as irradiated. On the other hand the wildlife in the evacuated region was left and in the years since 1986 has appeared unaffected by the radiation. Today it is thriving, freed from the imposition of human habitation, as shown in several intriguing videos that are available6. Evidently even in this, the worst possible civil nuclear accident, the death toll was moderate compared to many a major hydro, coal, oil or gas accident, and evidence of additional cancer, though much dreaded, is remarkably hard to find.
On the cities of Hiroshima and Nagasaki in 1945 two nuclear bombs were exploded. If nuclear radiation causes a significant death toll in later years through an increased rate of cancer, it should be evident here, especially as the radiation was emitted primarily as an acute flash giving least time for the benefit of response mechanisms. Certainly many died in the terrible wave of blast and fire, although it is surprising to learn of the man from Nagasaki who was caught in Hiroshima by the first bomb and then returned home to suffer from the second. He died only a few years ago at the age of 93. But little is learnt from individual cases and it is more useful to look at the fate of a substantial number of inhabitants. The health of all those who survived to 1950 has been monitored for 50 years and compared to those who were not irradiated. Doses have been calculated for 86,611 and the Table shows the number who died of cancer in 50 years, the number expected (from the un-irradiated) and the additional number that are then attributed to radiation-induced cancer [PR2004]. More details are discussed elsewhere [AL2009].
| cancer deaths | expected | additional | |
|---|---|---|---|
| solid cancers | 10127 | 9647 | 480 |
| leukaemia | 296 | 203 | 93 |
The estimated total number of cancer deaths caused by radiation is 573 or 6.6 per thousand survivors. Evidently radiation did cause extra deaths, but at a fraction of the underlying cancer rate. The evidence does not show that survivors with a dose less than 100 mGy had any risk of additional cancer and, to the surprise of all brought up in the Cold War period, there is no evidence to confirm that radiation caused any inherited genetic effects. Overall this estimate of 573 extra deaths in 50 years is less than 1% of those killed by the initial blast and fire.
The data can be used in the following way to estimate an upper limit to the number of workers at Fukushima who might die of cancer in the next 50 years. The 30 workers with the highest doses all received doses between 100 and 250 mGy, albeit spread over a year. At Hiroshima and Nagasaki 5949 survivors received an acute dose in this range and suffered an additional cancer death rate of 1 in 150 in the following 50 years. So at Fukushima the expected number of additional deaths is 1/150 times 30, that is 0.2, meaning that no death is likely.
6. The many sources of misunderstanding
Some do not accept these conclusions because they distrust the data. It is always possible to do that and on occasion it may be justified. But human society depends on trust. In fact among the worst effects of the Fukushima accident was the damage done to trust – trust in institutions, trust in science, as well as personal trust. If everyone distrusts others, life gets very bleak at the individual level and, collectively, the environment would only accommodate a tiny fraction of the world's current population. So, although we need to be discerning about the evidence we accept and should not rely exclusively on a single source, we should expect to find some compatibility between different sources in the search for credibility.
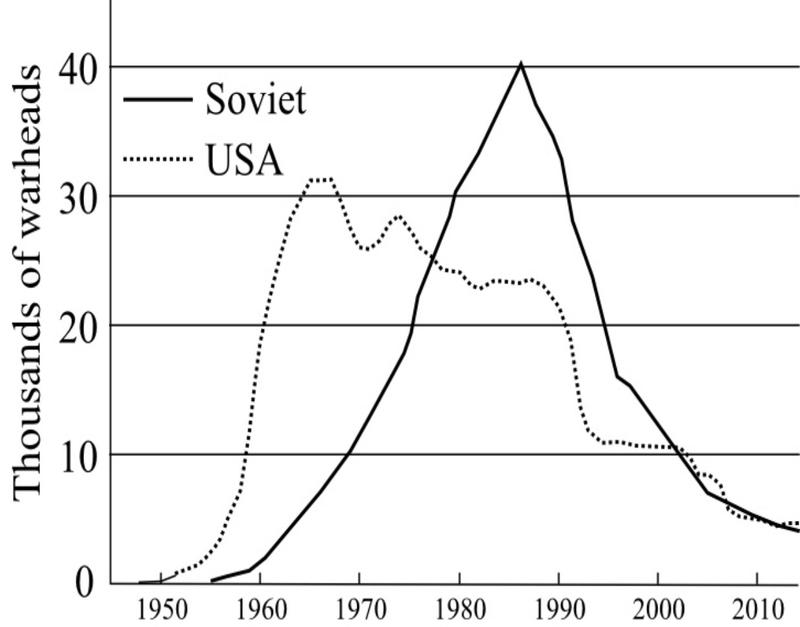
But there are other reasons why people disagree. These centre around personal preconceptions as well as educational, financial and legal pressures on individual opinion. These can be slippery and need constant examination. The strongest collective influence comes from history, in this case the experience of the Cold War and the nuclear Arms Race. Figure 3 shows how the number of warheads grew by tens of thousands, each one many times larger than the Hiroshima and Nagasaki devices. Furthermore these were tested in the atmosphere by both sides, resulting in worldwide radioactive fallout many times greater than that from Chernobyl. This period was one of widespread fear and dread. The only way to stop the race was to promote the threat of radiation as a danger seen as worse than a possible conflict with the Soviet Union. This tactic was successful – but it came at the expense of scientific truth. Nuclear weapons are dangerous because of the blast and fire they cause, but today few people understand that for 60 years we have been living with a lie – the lie that nuclear radiation is exceptionally dangerous.
Today anti nuclear opinion still embraces the lie and is now blind to this misjudgement. Many will pass on with their misbelief still intact, as suggested by Max Planck:
A new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die.
Fortunately there are quite a number of bright environmentalists who have understood their mistake. Some have made a full length professional video, Pandora's Promise [ST2013], that is well worth watching and explains why they changed their minds. But most members of the public simply remain frightened and reluctant to consider changing simple long-standing beliefs. As Tolstoy explained, this may be true whether they are intelligent or not:
The most difficult subjects can be explained to the most slow witted man if he has not formed any idea of them already; but the simplest thing cannot be made clear to the most intelligent man if he is firmly persuaded that he knows already, without a shadow of doubt, what is laid before him.
However the most insidious opposition comes from the radiation safety experts whose salaries, research funding and bureaucracy depend on the status quo, that is LNT-based regulations and the Precautionary Principle. They adhere to ALARA as if it were the Hippocratic Oath of their profession. Their basic reluctance to consider changing their opinion is captured by the words of Upton Sinclair:
It is difficult to get a man to understand something when his salary depends on his not understanding it.
Unfortunately it is to them that politicians and the media turn for expert guidance. The public tend to vote for safety by default and that is what this industry offers. The resulting demand for extra resources and protection, though not justified by any scientific evidence, make nuclear technology expensive without cause. Yet the influence of the ALARA-related emergency reactions to Fukushima has been extremely harmful to life, the environment and the economy, not only in Japan but around the world.
Particularly insidious is the effect of compensation paid to those involved in accidents. Courts of law do not seek to apply the laws of nature but those of precedent. Over-reaction to radiation exposure has involved the payment of very large sums without any hurt having been established. The quoted opinion of those seeking legal compensation in court cannot be trusted while the lips of those already given it are sealed. Where people have a poor understanding of the science, litigation, or the threat of it, has often acted to entrench ignorance and suppress the free discussion of evidence. Many argue over who was to blame for Fukushima, but the answer is nobody – it was a natural accident without casualties, except those caused by fear.
7. The safety of ionising radiation
Since high dose rates of ionising radiation can be injurious to life, the threshold for such injury needs to be found – that is a scientific question. Then a safe upper limit for regulatory purposes can be set somewhat below that threshold, taking into account social and other factors. These social factors should not be allowed to confuse discussion of the scientifically observed threshold. Special consideration for children and pregnant mothers are socially important but they should not affect the threshold unless the evidence actually indicates that.
According to ALARA there is no threshold and so the limit for any radiation exposure should be as low as possible in an attempt to appease public concern. That approach makes no reference to any evidence of demonstrated risk and was solely responsible for the disaster at Fukushima. That is wrong – the threshold should be based on evidence of harm to health.
There is an upper bound on a single acute dose that produces no injury in the region of 100 mGy, if received all at once as at Hiroshima and Nagasaki. But what does all at once mean? The injury from a dose received over a period, perhaps as long as a typical cell cycle or longer, is likely to benefit from biological repair mechanisms. So a threshold might be at a certain dose per day or per week – to be conservative we look at a threshold chronic dose per month, meaning that there is no evidence of injury from such a monthly dose when steadily repeated, month after month. What is known of the effect of 100 mGy per month as a steady dose rate? Human evidence for the effect of chronic dose rates is rare but other sources support a consistent story.
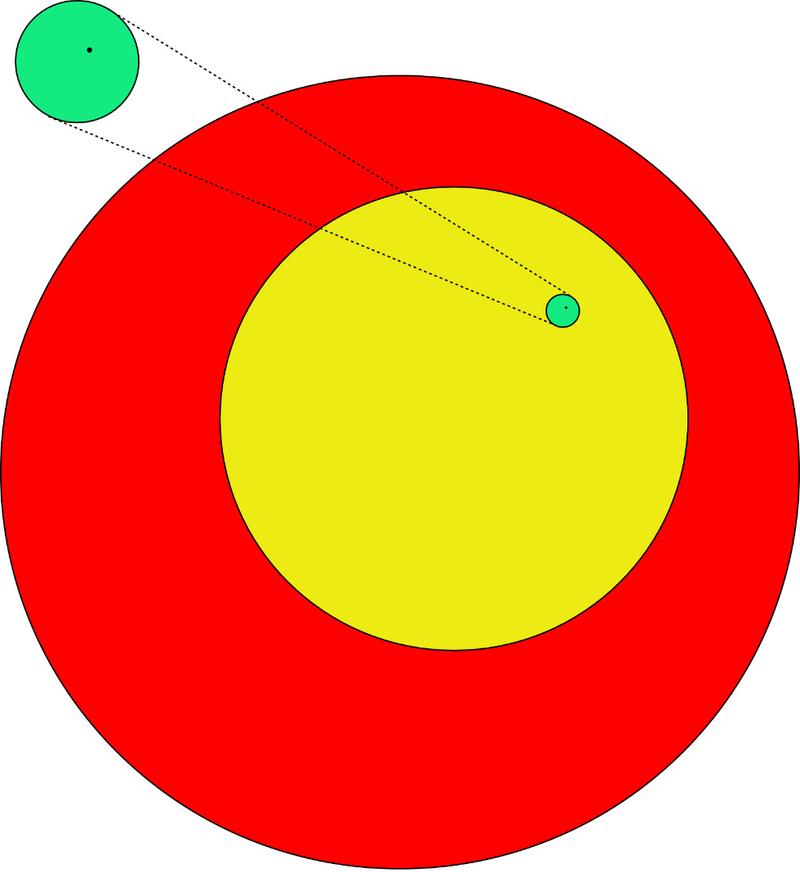
Graphical presentations are useful when reaching out to a wide audience. Monthly doses are shown pictorially in Figure 4 by the relative area of circles. The red circle is a monthly dose rate that kills the cells of a tumour in therapy and so is well above the threshold. However the yellow circle describes a dose accepted by the general public to healthy tissue near a treated tumour from which there is usually full recovery. It is a large dose of about 30,000 mGy per month. Although it does cause cancer occasionally and is not repeated, patients who receive it usually return home with improved life expectancy. Nevertheless it too is above threshold. The area of the black dot inside the green circle represents the ALARA-based ICRP recommendation for public safety (1 mGy per year or 0.08 mGy per month), a quarter of a million times smaller than the yellow one. If an acute dose of 100 mGy is harmless and most repair and replacement mechanisms are effective within a month, then a dose of 100 mGy per month should be harmless: this is shown as the green circle, 1000 times larger than the dot and 200 times smaller than the yellow circle. What other human data are relevant?
Some of the Radium Dial Painters received life doses of radium to their bones [RO1994]. These showed a clear threshold for bone cancer after life-time doses of 10,000 mGy. It is known that alpha radiation from radium is substantially more carcinogenic than other forms. Nevertheless this threshold is not qualitatively inconsistent with 100 mGy per month, the green circle. Data on dogs given gamma radiation at 3 mGy per day (100 mGy per month) throughout their lives show no difference in mortality when compared to a control group over 8 years [FR2002]. Dogs' lifespan is much longer than mice and mortality data covers all fatal diseases, not just cancer. This matches the green circle too. Further support comes from genetic studies on mice. These work with genetically identical mice and can detect the presence of DNA errors so skipping the latency period. Recent results with mice treated chronically with 3 mGy per day for five weeks showed no genetic changes [OL2012].
Whether the higher mortality of painters above 10,000 mGy and the dogs at an age greater than 8 years is due to ageing of the immune system or a threshold for whole-of-life dose is a moot point. Anyway any effective threshold for whole-of-life dose is greater than 5,000 mGy, a figure not inconsistent with the rate of second cancers among children who received radiotherapy for a first cancer [TU2011]. It may turn out that there is no such threshold and that later failure is best characterised by the state of the immune system.
Historically, the threshold for radiation injury, seen as a safe level, was agreed in 1934 at 2 mGy per day, substantially the same as the green circle of Figure 4. In his Sievert Lecture of 1980 Lauriston Taylor7 said [TA1980]
Today we know about all we need to know for adequate protection against ionizing radiation. Therefore, I find myself charged to ask: why is there a radiation problem and where does it lie? No one has been identifiably injured by radiation while working within the first numerical standards [2mGy/day] set by the NCRP and then the ICRP in
- An equally mischievous use of the numbers game is that of calculating the number of people who will die as a result of having been subjected to diagnostic X-ray procedures. An example of such calculations are those based on a literal application of the linear non-threshold dose-effect relationship, These are deeply immoral uses of our scientific knowledge.
8. Conclusions
Evidence suggests that life has achieved natural dynamic protection against the damaging effects of ionising radiation and this is responsive in a way that compliance with mere regulation could never be. Widespread education with genuine explanation is needed to give everybody the necessary guidance and reassurance. This is what is done already for the more serious example, ultraviolet radiation from the Sun. This radiation lies next to X-rays in the radiation spectrum: it too causes cell death (sun burn) and cancer at high dose rates. Some 9000 people a year die from skin cancer in the USA but family advice from pharmacists and doctors offers acceptable guidance without panic or appeal to international committees.
Humans became dominant on planet Earth by studying the many threats to life, and then communicating their findings to others in society. In the case of nuclear energy science has failed to do this, instead advocating simply that all should avoid exposure to it. Consider fire as another example and imagine the scene long ago when environmentalists objected to an early proposal to bring fire into the home. They were right about the dangers in that case, but it was essential to a better life and they were wrong to oppose it. Today, on the proposal that nuclear energy should replace fire, opposition is mistaken on both counts – it is safe and it is essential for the environment and human survival.
Today there is a need for both bottom-up education and also a top-down change of regulations. I am a member of a group of scientists from Canada, the US, Poland, New Zealand and elsewhere who publicise the scientific, medical and political case for proper science-based radiation regulations in clinical medicine and nuclear technology [SARI]. Three petitions have been made to the US Nuclear Regulatory Commission to relax limits and I have made a submission to UK Parliamentary Select Committee [AL2016].
Radiation and nuclear were propaganda words successfully used to frighten the populace during the Cold War. The message that such science is complicated and only for eggheads in secret bunkers was all part of the propaganda. For 70 years society has accepted without justification that nuclear technology is an exceptionally fearsome and ghoulish aspect of nature. We have allowed society to drift, assimilating what it is told into worn-out views rather than thinking matters out afresh. As President Kennedy pointed out, new thoughts are more uncomfortable than old views:
The great enemy of the truth is very often not the lie – deliberate, contrived and dishonest – but the myth – persistent, persuasive and unrealistic. Too often we hold fast to the cliches of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.
Perhaps our children will open their eyes and show more sense than we have done. Nuclear safety is not just a matter for engineering and physics, but for education, social psychology and an appreciation of the marvels of biology. Fear of radiation is currently preventing the choice of an economic and sustainable environment, and unwarranted regulation continues to strangle obvious developments in the nuclear industry. This is a tragedy for the unwitting consumer and for the environment. We need more education, less regulation, more safe cheaper nuclear power stations and fewer international radiation committees.
References
[AL2006] Allison W Fundamental Physics for Probing and Imaging OUP ISBN 9780199203888
[AL2009] Allison W Radiation and Reason: the Impact of Science on a
Culture of Fear
ISBN 9780956275615
www.radiationandreason.com
[AL2011] Allison W BBC Viewpoint: We should stop running away from radiation www.bbc.co.uk/news/world-12860842
[AL2015] Allison W Nuclear is for Life: A Cultural Revolution ISBN 9780956275646 www.nuclear4life.com
[AL2016] Allison W Submission to House of Commons Science and Technology Select Committee http://data.parliament.uk/writtenevidence/ ... /science-advice-for-chemical-biological-radiological-or-nuclear-emergencies/written/33322.html
[AN2009] Angell M www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
[FR2002] Fritz TE The influence of dose, dose rate and radiation quality on the effect of protracted whole body irradiation of beagles. Brit J Radiol suppl 26: 103-111
[HE2016] Henriksen T Radon, lung cancer and LNT http://go-nuclear.org/radiation/item/978-radon-lung-cancer-and-lnt-model-thormod-henriksen-biophysics-and-medical-physics-group-u-of-oslo
[HO2016] Horton R www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(15)60696-1.pdf
[IA1988] IAEA *The Radiological Accident in Goiania,
*www-pub.iaea.org/mtcd/publications/pdf/pub815_web.pdf
[IA1998] IAEA Dosimetric ... radiological accident in Goiânia in
1987,
www-pub.iaea.org/MTCD/publications/PDF/te_1009_prn.pdf
[ICR2007] International Commission for Radiological Protection Report 103, www.icrp.org
[LE2015] Leuraud K, Richardson DB, Cardis E et al, Ionising radiation and risk of death from leukaemia and lymphoma in radiation monitored workers: an international cohort study. Lancet Haematol 2(7):e276–e281
[MU2009] Muirhead CR et al. Mortality and cancer incidence following occupational radiation exposure: third analysis of the National Registry for Radiation Workers. British Journal of Cancer, 100, 206–212.
[MU1915] Murphy JB and Morgan JJ The effect of Roentgen Rays on the rate of growth of spontaneous tumours in mice Rockefeller Institute for Medical Research www.ncbi.nlm.nih.gov/pmc/articles/PMC2125377/pdf/800.pdf
[MU1920] Murphy JB The effect of physical agents on the resistance to mice of cancer Rockefeller Institute for Medical Research www.pnas.org/content/6/1/35.full.pdf+html
[OL2012] Olipitz et al Integrated Molecular Analysis Indicates Undetectable Change in DNA Damage in Mice after Continuous Irradiation at ~ 400-fold Natural Background Radiation, ehp.niehs.nih.gov/1104294/ and newsoffice.mit.edu/2012/prolonged-radiation-exposure-0515
[PR2004] Preston, Dale L et al Effect of Recent Changes in Atomic Bomb Survivor Dosimetry on Cancer Mortality Risk Estimates. Radiation Research. 162: 377–389.
[RI2015] Richardson DB, Cardis E, Daniels RD et al, Risk of cancer from occupational exposure to ionising radiation: retrospective cohort study of workers in France, the United Kingdom, and the United States. BMJ. doi:10.1136/bmj.h5359
[RO1994] Rowland RE, Radium in Humans, A Review of US Studies.
ANL/ER3 www.osti.gov/accomplishments/documents/fullText/ACC
0029.pdf
with comment (2004)
www.rerowland.com/Dial_Painters.pdf
[SARI] www.radiationeffects.org
[SA2016] Sacks W, Meyerson G and Siegel JA, Epidemiology without biology: Biology: False Paradigms, Unfounded Assumptions, and Specious Statistics in Radiation Science Biol. Theory http://link.springer.com/article/10.1007/s13752-016-0244-4
[ST2013] Stone R. Documentary Pandora's Promise http://pandoraspromise.com/
[TA1980] Taylor LS. The Sievert Lecture 1980. Some Non-Scientific Influences Radiation Protection Standards and Practice in Radiation Protection: A Systematic Approach to Safety. Proc. 5th Congress of the International Radiation Society. Pergamon Press. pp 3-15.
[TU2011] Tubiana M et al A new method of assessing the
dose-carcinogenic effect ...
Health Phys 100, 296
(2011)
[VA2013] Nelson Valverde, private communication
[WE2015] Observations by Tony Weidberg reported in a blog posted by the Cato Institute www.cato.org/blog/you-ought-have-look-case-against-modern-science
[WH2006] World Health Organization Health effects of the Chernobyl accident and Special Health Care Programmes. whqlibdoc.who.int/publications/2006/9241594179_eng.pdf
Footnotes
-
The probability of a result being due to a random fluctuation alone: of 1 sd is 1/3; of 2 sd is 1/20; of 3 sd is 1/370; of 4 sd is 1/16,000; of 5 sd is 1/1,750,000. The habit of describing 2 sd as a firm conclusion should cease. ↩
-
This example was not chosen at random: it was commended to the author in January 2011 by an adherent of the Linear No-Threshold (LNT) Model as compelling evidence for it. ↩
-
Einstein wrote three papers in 1905, each of which might have earned him a Nobel Prize. These were the Special Theory of Relativity, the theory of Brownian Motion and the Photoelectric Effect. When he was awarded the 1921 prize, it was for the Photoelectric Effect, not the Theory of Relativity for which he is popularly more famous. ↩
-
These numbers are simplified to focus attention on the important qualitative aspects of what is happening. ↩
-
Radiation from earth-bound radioactivity was 2 or 3 times higher because less of the thorium and uranium in rocks had decayed away. Radiation from space may also have been higher or lower on account of variations in the shielding effect of the atmospheric density and the terrestrial magnetic field. ↩
-
For example a video on Chernobyl wildlife (2012) Discovery Channel http://t.co/puM2rwyBMH, also at https://www.youtube.com/watch?v=IEmms6vn-p8 and triggered pictures of wildlife at Chernobyl (2015) http://www.bbc.co.uk/news/science-environment-32452085. ↩
-
Physicist (1902-2004), charter member of ICRP (1928), founder and chairman of US NCRP for 48 years. ↩